

The Missing Key: Why Magnesium Determines Whether Your Vitamin D Works
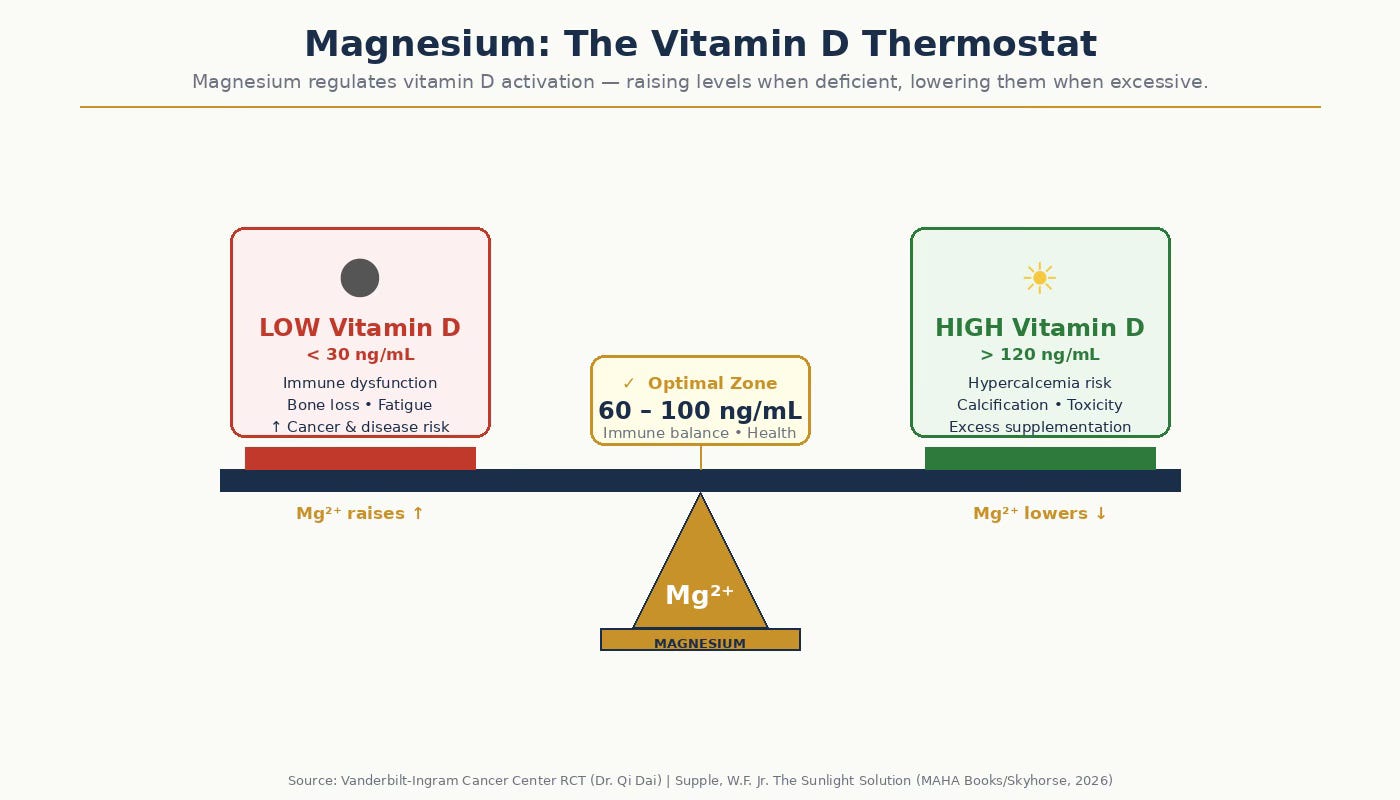
Most people supplementing with vitamin D are doing so without the cofactor that makes it functional. Magnesium acts like a Vitamin D Thermostat.

You’ve tested your vitamin D. It came back low. You started supplementing — 5,000 IU a day, maybe more — and months later the level hasn’t budged much. Or it has budged, but you still feel the same. You’re not alone, and there’s a specific reason this happens to a surprisingly large number of people.
The reason is magnesium.
Vitamin D Is Not Ready to Use Out of the Box
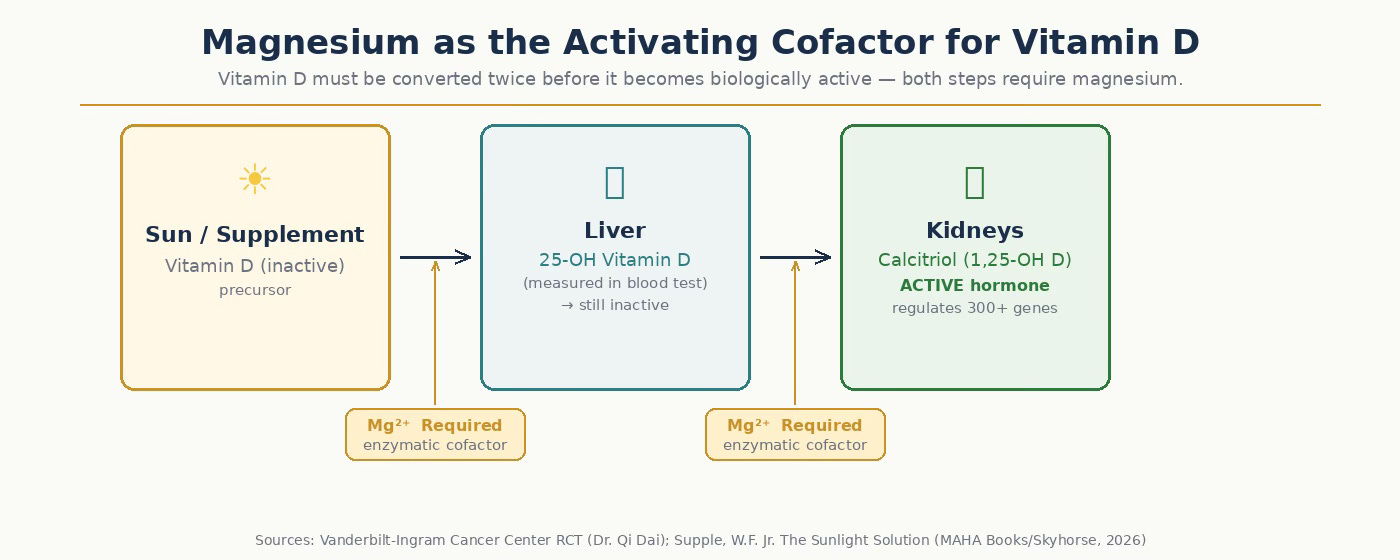
When you take a vitamin D supplement — or produce vitamin D through sun exposure — what enters your bloodstream is not the active, functional form. It’s a raw material, a precursor that has to be chemically transformed before your body can actually do anything with it.
The journey looks like this: the vitamin D from your supplement travels to the liver, where enzymes convert it into 25-hydroxyvitamin D (25-OH D) — the form measured in your standard blood test, the number your doctor reads as your “vitamin D level.” But that form is still inactive. It then travels to the kidneys, where a second enzymatic conversion produces 1,25-dihydroxyvitamin D, also called calcitriol — the biologically active hormone that actually enters your cells, binds to vitamin D receptors, and does the work of regulating calcium absorption, immune function, and gene expression across more than 300 target genes.
Both of those conversion steps require magnesium as an essential cofactor.
Without adequate magnesium, the enzymatic machinery that drives these conversions slows or stalls. You can take vitamin D every day, maintain a serum 25-OH D level that looks perfectly acceptable on paper, and still have your body failing to produce adequate calcitriol — the form that actually matters. The blood test looks fine. The biology isn’t working.
What Vanderbilt Found
Researchers at the Vanderbilt-Ingram Cancer Center ran a randomized controlled trial specifically examining the relationship between magnesium and vitamin D status — and the findings were striking enough to reframe how the two nutrients should be understood.
What they found was that magnesium functions as a biological thermostat for vitamin D. It raised vitamin D levels in people who were deficient while simultaneously reducing vitamin D levels in those whose levels were already elevated. This bidirectional regulatory effect suggests that magnesium doesn’t simply push vitamin D in one direction — it helps calibrate it. The lead researcher, Dr. Qi Dai, characterized magnesium as “the missing key to keeping vitamin D levels in balance.”
This finding carries significant implications for interpreting the mixed results that have plagued vitamin D research for decades. Studies showing robust vitamin D benefits have coexisted uneasily alongside trials showing minimal or null effects. If a substantial portion of study participants were magnesium-deficient — and therefore unable to fully activate the vitamin D they were receiving — the vitamin D intervention would appear less effective than it truly is. The inconsistency in the literature may not reflect inconsistency in vitamin D’s biology. It may reflect uncontrolled magnesium status across study populations.
The Scale of the Problem
Roughly 50% of Americans consume a magnesium-deficient diet. The recommended daily intake is 420 mg for men and 320 mg for women. The average American diet delivers approximately half of that.
Magnesium is concentrated in foods that have been systematically displaced from the modern diet: leafy greens, nuts, seeds, whole grains, legumes, dark chocolate. These are not foods that anchor a standard Western diet. And here is the particular irony: many people who are vitamin D deficient are vitamin D deficient precisely because of dietary and lifestyle patterns — limited sun exposure, limited intake of fatty fish, limited consumption of fortified foods — and those same patterns tend to be low in magnesium as well. The nutrient gap that prompts the vitamin D supplement is the same gap that prevents the supplement from working properly.
Why This Matters Beyond Blood Test Numbers
The connection between vitamin D and immune function has become an area of intense clinical interest. Research from the PROVIDENCE study — a prospective trial of 164 cancer patients receiving immune checkpoint inhibitor therapy — found that 94.1% of patients had vitamin D levels at or below 30 ng/mL at the start of treatment. When those patients received systematic vitamin D repletion, their outcomes improved significantly: longer overall survival, longer time to treatment failure, higher disease control rates.
A separate Brazilian randomized controlled trial published in 2025 found that just 2,000 IU of vitamin D daily during breast cancer chemotherapy produced a 79% improvement in pathological complete remission rates compared to placebo.
Imagine the results if the physiologically more relevant dose of 5,000 IU per day were used.
These are substantial effects. But neither study formally controlled for magnesium status. If some portion of participants failed to fully activate the vitamin D they received — because they remained magnesium-insufficient — the effects observed may represent an underestimate of what vitamin D repletion can actually achieve when the full conversion pathway is supported.
The Practical Hierarchy
If you are supplementing with vitamin D, or considering it, the intervention is most likely to work when approached in this sequence:
First, know your level. A 25-OH D blood test is straightforward, inexpensive, and covered by most insurance when there is clinical indication. The conventional threshold for sufficiency is 30 ng/mL; researchers focused on immune and cancer outcomes generally favor 60-100 ng/mL as the target range.
Second, assess your magnesium intake. This does not necessarily require a blood test — serum magnesium is a poor indicator of total body magnesium stores, as most magnesium is intracellular. A more useful exercise is to honestly evaluate dietary intake. Are leafy greens, nuts, seeds, and legumes genuinely present in your daily eating? If not, the gap is real and worth addressing.
Third, close the magnesium gap through food where possible. A handful of almonds (roughly 80 mg), a cup of cooked spinach (roughly 157 mg), a quarter cup of pumpkin seeds (roughly 190 mg) — magnesium is accessible in whole foods in meaningful amounts. This approach also provides cofactors beyond magnesium that support overall nutritional status.
Fourth, consider magnesium supplementation if dietary closure is not realistic. Magnesium glycinate and magnesium citrate are the most bioavailable and best-tolerated oral forms. They are generally taken with food; many people find magnesium glycinate particularly calming and prefer it in the evening. Standard supplemental doses range from 200–400 mg elemental magnesium per day. If you have kidney disease, discuss magnesium supplementation with your physician before starting, as impaired kidneys cannot clear excess magnesium efficiently.
A Note on the Research Landscape
The magnesium-vitamin D connection represents exactly the kind of nutrient interaction that tends to be systematically underweighted in clinical research design. Trials are built around single interventions with clearly measurable primary endpoints. The messy reality that one nutrient’s activity depends on the status of another rarely gets accounted for at the protocol level.
This is part of a larger problem in how vitamin D research — and nutritional research generally — has been conducted. As documented in a upcoming article on vitamin D as an uncontrolled variable in pharmaceutical trials, the immunological effects of vitamin D sufficiency versus deficiency are substantial enough to change the apparent efficacy of drugs tested across those two populations. When magnesium status is added as a second uncontrolled variable layered on top of vitamin D status, the complexity compounds.
The practical takeaway is not to wait for research designs to catch up. The safety profiles of both vitamin D and magnesium supplementation at recommended levels are well established. The biological rationale for ensuring both are adequate is clear. And the cost of addressing both — in time, money, and effort — is low relative to the potential benefit.
Getting your vitamin D tested is step one. Making sure you have the biochemical infrastructure to activate it is step two. Most people who take vitamin D supplementation seriously have done step one. Many have not done step two.
William F. Supple, Jr., PhD, is the author of the upcoming book, The Sunlight Solution: Reclaiming Vitamin D, Reversing the Chronic Disease Epidemic, and Making America Healthy Again (MAHA Books/Skyhorse, 2026).
Sources:
Vanderbilt-Ingram Cancer Center RCT on magnesium and vitamin D regulation (Dr. Qi Dai, lead researcher)
Omodei, M. S., et al. (2025). Vitamin D Supplementation Improves Pathological Complete Response in Breast Cancer Patients Undergoing Neoadjuvant Chemotherapy: A Randomized Clinical Trial. Nutrition and Cancer, 77(6), 648–657.
Kouchaki, E., et al. (2023). Systematic vitamin D supplementation is associated with improved outcomes and reduced thyroid adverse events in patients with cancer treated with immune checkpoint inhibitors: Results from the prospective PROVIDENCE study. Cancer Immunology, Immunotherapy, 72(10), 3261–3274.
Supple, W. F., Jr. (2026). The Sunlight Solution. MAHA Books/Skyhorse

Included in all posts
General Recommendations for Vitamin D for Healthy Adults
The U.S. Institute of Medicine (IOM), now the National Academy of Medicine, recommends a dietary reference intake of 600 IU (International Units) per day for adults up to age 70, and 800 IU for those over 70, to maintain bone health (Institute of Medicine, 2011). However, this amount is orders of magnitude too low considering that the human body “uses” at least 4000 IU vitamin D per day.
However, there is a vast literature on the extraskeletal functions of vitamin D for maintaining optimal functioning of the immune system, muscular system and ideal aging that indicates that optimal levels of serum vitamin D are much, much higher (e.g., Grant et al. 2020).
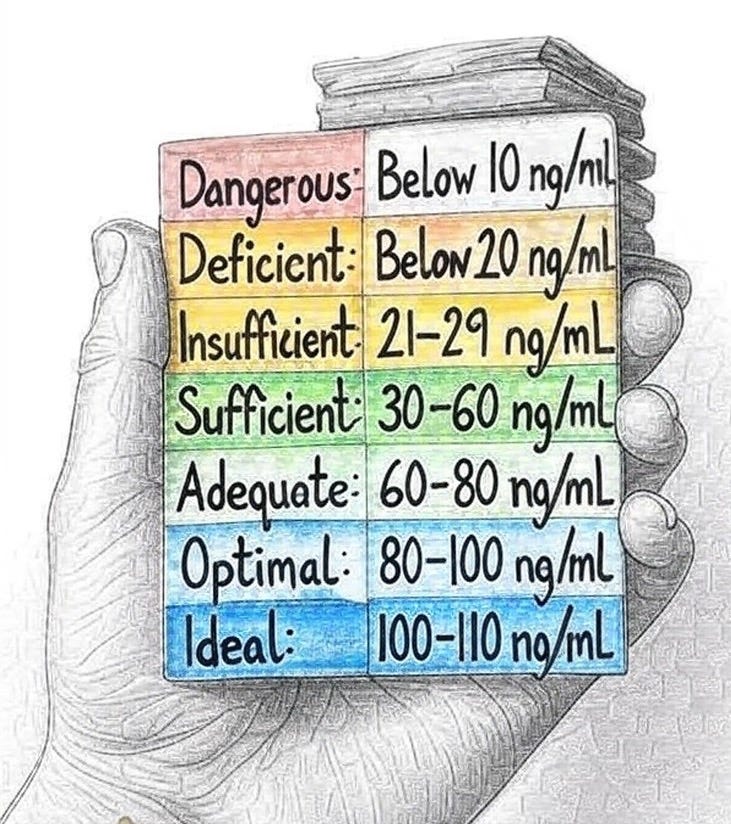
Based on Blood Levels
A blood test provides a clear picture of vitamin D status. Levels are typically categorized as follows (Holick et al., 2011; Wang et al., 2017):
Link to StarPowerLifeSciences.org for more information
RBC magnesium provides a better reflection of body stores of magnesium. Desired value is in the top half of the reference range.
While recently in hospital for appendectomy, serum mag levels were low and I was given IV mag daily. The internal med dr commented, well, hospital diets aren't very high in magnesium. And I said, well, most foods nowadays are low in magnesium. I don't think he even noticed.
On my day of discharge, I had to explain to my nurse that the mag oxide pill she came in to give me for my "low magnesium" wasn't going to do anything for my magnesium levels and had been ordered a few days prior to help with post-op ileus.
What about the action of K2 on Vit D 3 supplementations?